Publication
Article
Article
Author(s):
As a breast cancer survivor and patient advocate, I (Maimah Karmo) understand what it feels like when a cancer journey takes an unexpected turn. Over the years, I have spoken with many patients who have been told by their physicians that their tumor’s biology had changed—new “typos” had appeared in the DNA instruction manual of their cancer cells. These genetic mutations had, in effect, “changed the locks” on the cells’ doors, enabling them to evade treatments that had previously been effective.
Today, advances in research, diagnostic technologies, and targeted therapies make it possible to identify these changes and offer patients renewed hope. Drawing on nearly 2 decades of patient advocacy experience, I have partnered with Eleonora Teplinsky, MD, head of breast and gynecologic medical oncology at Valley-Mount Sinai Comprehensive Cancer Care to share practical strategies for helping patients understand ESR1 mutations—what they are, why they matter, and how new diagnostic tools and treatment options are reshaping care.
Understanding ESR1: Genes, Hormones, Receptors, and the Lock-and-Key Model
The ESR1 gene encodes the estrogen receptor α (ERα), a critical hormone receptor that mediates estrogen-driven growth in many breast cancers. Conceptually, ESR1 can be viewed as the genetic blueprint that produces the cellular “lock” represented by the estrogen receptor, while estrogen functions as the “key” that binds and activates this receptor. When estrogen binds to the receptor, ERα promotes the proliferation and survival of cancer cells. In hormone receptor– positive breast cancer, malignant cells exploit this pathway to sustain tumor growth and progression.
Endocrine therapies are designed to interrupt this process by either removing the key or changing the lock. Aromatase inhibitors lower estrogen levels in the body, effectively taking away the key, while drugs like tamoxifen bind directly to the receptor—blocking the keyhole—so estrogen cannot activate it. This prevents the hormonal growth signal from triggering the cancer cells to grow.
However, after a prolonged period on endocrine therapy, cancer cells can develop mutations in the ESR1 gene that change the shape of the estrogen receptor—the lock itself. These changes often occur in the receptor’s key binding area, allowing it to turn “on” without the key. In other words, the lock is altered so that it can open on its own, bypassing the need for estrogen altogether. In effect, the cancer has found a way to open the door despite our efforts—an acquired resistance mechanism that emerges under the selective pressure of hormonal therapy.1,2
Crucially, ESR1 mutations are rare in treatment-naive, primary breast cancers (≈1%) but are more common in metastatic, endocrine-resistant disease that has stopped responding to hormonal therapy (10%–50%).1 Studies demonstrate that up to about 40% or 50% of women with metastatic ER+/ HER2– breast cancer will develop an ESR1 mutation following exposure to 1 or more lines of hormone therapy.3,4,5 Clinically, this underscores the dynamic evolution of tumor biology under therapeutic pressure. Explaining this to patients, one might say: “The biology of your tumor can change over time. After prolonged hormone treatment, new receptor mutations may arise that reduce the effectiveness of therapies that previously controlled your cancer.”
How ESR1 Mutations Develop and Drive Resistance
ESR1 mutations are acquired adaptations that emerge as cancer cells are repeatedly challenged by endocrine therapy. For example, when a patient has been on an aromatase inhibitor— which reduces estrogen levels and effectively removes the key from the system—for an extended period, resistant cancer cell clones with altered estrogen receptors can arise.
A useful way to explain this to patients is to say: “Imagine a locksmith constantly changing the tumblers inside a lock each time you try a new key. Eventually, the original key no longer fits.” Another way to describe it is: “Even if estrogen levels are low, the estrogen receptor stays turned on—it no longer needs estrogen to drive cancer cell growth.” This adaptation renders the tumor resistant to therapies designed to block or suppress estrogen.
Clinically, this resistance is reflected in shorter durations of response to subsequent endocrine therapies among patients whose tumors harbor ESR1 mutations. These mutations are a well-established mechanism of endocrine resistance. Organizations such as the American Society of Clinical Oncology (ASCO) recognize ESR1 mutations as a form of “adaptive endocrine resistance.”6 Essentially, these mutations reprogram the cellular lock so that the tumor can continue to grow despite low estrogen levels or the presence of other therapies. As Dr. Kalinsky notes, patients with ESR1-mutated tumors typically do not benefit from standard aromatase inhibitors—it’s akin to using an old key on a newly altered lock.2
From a patient-communication perspective, the analogy continues: If endocrine therapy is the key that locks the cancer cell door, an ESR1 mutation acts like an unexpected shortcut that pops the door open and keeps it open. The old key (hormone therapy) no longer works effectively on this new lock. Importantly, these mutations are often subclonal and evolve over time, meaning that different tumor regions or metastatic sites may acquire mutations at various points in time. This dynamic nature underscores the importance of testing at every point of disease progression, a practice strongly recommended by ASCO.6
The Impact on Treatment Selection and Disease Course
The presence of an ESR1 mutation has significant clinical implications, primarily because it can render standard endocrine therapies ineffective. Clinicians should be aware that when a patient’s disease progresses on first-line hormone therapy (often given alongside a CDK4/6 inhibitor), up to nearly half of these cases may involve the emergence of an ESR1 mutation.7
From the patient’s perspective, this can be explained as: “We have found a specific mutation that made the previous treatment less effective. Fortunately, there are now targeted therapies available that can improve outcomes in this situation.” One such option is elacestrant, an oral selective estrogen receptor degrader (SERD) that targets and degrades the estrogen receptor, even when it has been altered by an ESR1 mutation. This provides a valuable new treatment approach for patients whose cancers have developed resistance to standard endocrine therapies.
Preclinical data further support these clinical findings. ESR1 mutations lead to receptors that are constitutively active, meaning they continue to signal for tumor growth even when estrogen is blocked.1,2 This contributes to a more aggressive disease course, with tumors harboring ESR1 mutations often progressing more rapidly.
For clinicians, the detection of an ESR1 mutation should signal a clear need to adjust the treatment strategy. At this clinical juncture, therapies that degrade the estrogen receptor (SERDs) or combine targeted agents move to the forefront of care. Current recommendations support making this transition at the time of confirmed disease progression.8
The Vital Role of Genomic Testing and Liquid Biopsy
Given the adaptive nature of ESR1 mutations, timely genomic testing is essential to capture changes in a patient’s tumor biology. For this reason, genomic profiling is recommended at each point of metastatic disease progression. ASCO’s recent guideline updates explicitly advise testing for ESR1 mutations at each metastatic progression.6 Dr. Kalinsky emphasizes that this testing should occur only after patients have received endocrine therapy, not at initial diagnosis.6 This recommendation aligns with both FDA and National Comprehensive Cancer Network® (NCCN®) guidance. NCCN now advises assessing ESR1 status at progression using nextgeneration sequencing (NGS) or polymerase chain reaction (PCR) on blood samples (to detect circulating tumor DNA, or ctDNA) rather than relying on archived tumor tissue, which cannot detect mutations acquired over time.9
Liquid biopsy (testing ctDNA from blood) is generally preferred. One reason is that ESR1 mutations can vary across different metastatic sites; a single tissue biopsy may miss certain subclones, while ctDNA offers a more comprehensive snapshot of tumor DNA throughout the body.10 In addition, evidence suggests that liquid biopsy is more sensitive for detecting ESR1 mutations. Archived primary tumor samples seldom contain these mutations (often <1%),1 so relying on older tissue can be misleading. If fresh tissue is obtained at progression, however, ESR1 testing remains an option.
Clinicians should also prepare patients for the possibility of this testing. A simple way to explain this is: “We may need a blood test the next time your cancer grows to see if the tumor’s DNA has changed.” In practice, if disease progression occurs while a patient is receiving endocrine therapy, a plasma sample is collected and sent for a NGS panel or a validated companion diagnostic.
Looking ahead, technology is making testing even more streamlined. For example, Menarini’s Stemline Therapeutics has partnered with Tempus to embed AI-driven alerts in electronic health records (EHRs), prompting oncologists to test for ESR1 mutations when clinically indicated.4 Similarly, Guardant360 offers an FDA-approved liquid biopsy assay specifically for detecting ESR1 mutations.11,12
In short, every eligible patient should undergo ESR1 testing at the time of disease progression, making it as integral to personalized cancer care as checking HER2 status. For patients, this can be explained simply: “Just as we regularly check your blood counts or heart function, we can also check your tumor’s DNA to identify new mutations as they appear. This allows us to choose the most effective next treatment.”
Anticipating Questions and Addressing Barriers
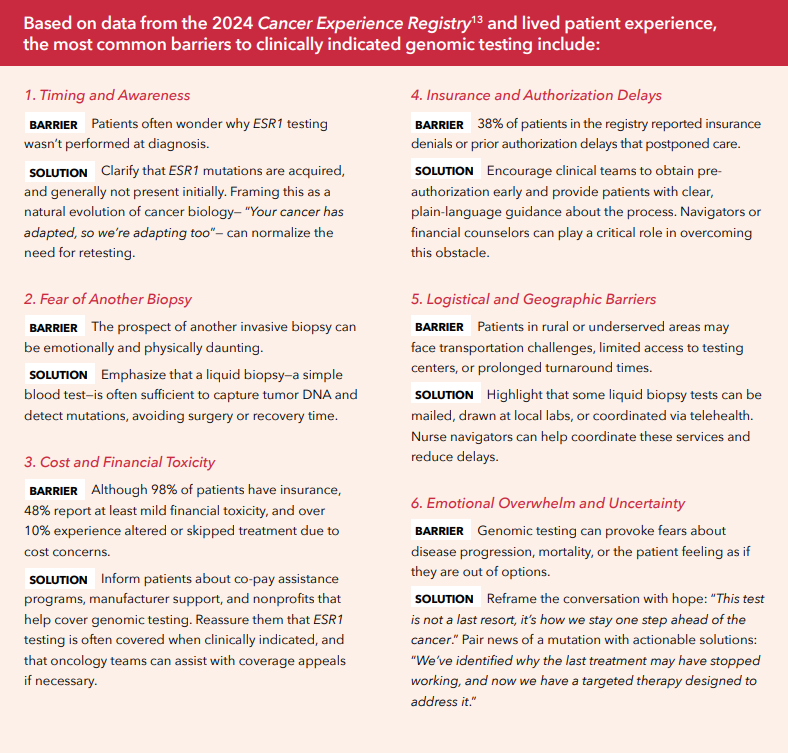
For patients living with metastatic breast cancer, genomic testing can feel like entering unfamiliar terrain, especially when they learn that their cancer may have changed. Common questions include:
These concerns are valid and reflect deeper issues around trust, access, cost, and understanding of the purpose of retesting. Explaining that ESR1 mutations typically emerge over time—often after a year or more of endocrine therapy—helps patients appreciate why testing at progression is standard practice. It’s not that something was missed earlier; rather, the tumor has evolved, and we must adapt accordingly.

Validating patients financially, emotionally, and logistically helps them feel seen and supported. As one survivor shared during a Tigerlily Foundation workshop, “I just wanted to know someone had a plan—and that I wouldn’t be the one falling through the cracks.”
That plan begins with proactive communication. Oncologists, nurses, and navigators should introduce the concept of ESR1 testing early when endocrine therapy begins, normalize the idea of re-testing at progression, and provide clear, compassionate explanations. For many patients, knowledge is power—and testing represents hope.
Communicating With Patients: Clarity, Compassion, and Analogies
Discussing ESR1 mutations can be daunting for patients, especially if they’re hearing for the first time that their cancer has changed. Technical terms like ligand binding domain or circulating tumor DNA offer little comfort in that moment. Instead, use plain language and concrete analogies.
As mentioned above, the lock-and-key analogy is one many patients understand: “Our original treatments worked because your cancer’s lock needed estrogen’s key to open the door and grow. Now the cancer has changed the lock. It can open the door even without estrogen.”
Another approachable explanation is to describe the mutation as a typo in the cancer’s instruction manual: “Imagine your cancer cells have an instruction booklet. Originally, the instructions said, ‘Only grow when estrogen is present.’ A mutation is like a typo that removes that rule, so the cells grow even when we take away estrogen. The good news is, we can find that typo with a simple blood test and use a treatment to target it.”
It’s also important to normalize retesting. Patients may not realize that treatment plans can and should change as the cancer evolves. Reframe testing as proactive care, not a sign of failure: “Each time we see new growth, we get another look at the tumor’s DNA—like checking an updated map. Each new map may show new flags (mutations), and our job is to spot them so we can choose the right next treatment.” Reassure patients that in many cases, this can be done with a blood test rather than another invasive biopsy.
Emotionally, acknowledge both frustration and hope. Patient advocates like Tigerlily emphasize that knowledge is power. When a patient learns they have an ESR1 mutation, pair that information with a clear next step. As Dr. Teplinsky might put it: “The test found the reason for disease progression, and we can start you on a therapy that specifically targets or attacks this mutation.”
Throughout the discussion, use collaborative language. Phrases like “we have learned” or “we can now do” rather than “your cancer has done this” keep the tone constructive and empowering. For example: “We’ve discovered something important about your cancer that can guide our next step. We’re going to check the tumor’s DNA to see if an ESR1 mutation is present, because if it is, we have a drug that works well for tumors like yours.”
Ongoing Care and Genomic Vigilance
Metastatic ER+/HER2– breast cancer care is shifting rapidly. As Dr. Teplinsky has noted, “We have moved from a one-size-fits-all approach to truly precision care.” That means genomic testing should be a routine part of disease monitoring, not a last resort. Whenever disease progression is observed, tumor DNA should be reassessed. If an ESR1 mutation is identified, flag it promptly and evaluate options, including approved therapies and relevant clinical trials.
While research continues with new SERDs and targeted therapies are on the horizon, effective, approved treatments are already available today. Industry efforts—such as Menarini’s partnerships with Tempus and Guardant— are helping ensure patients receive timely molecular testing. As industry leaders describe it, research efforts have delivered: “the first-ever therapy targeting ESR1 mutations… and a blood-based companion diagnostic.”11,12
From an operational standpoint, clinics can strengthen their readiness by:
In patient workshops I’ve co-led, one phrase resonates: “You only need one mutation to change everything.” That simple statement helps patients understand that even a small change in their cancer’s DNA can open the door to a different (and potentially more effective) treatment.
Conclusion: Staying Ahead With Knowledge and Communication
In an era of personalized oncology, ESR1 mutation testing and targeted therapy exemplify how science can directly improve patient outcomes. But the real value lies in how effectively this impact is explained to patients and caregivers. Clear, compassionate conversations turn a complex concept like ESR1 testing into an empowering moment.
Inform patients that ongoing testing is a sign of vigilant, proactive care, not cause for alarm. Use analogies, invite questions, and connect results directly to actionable next steps. As Dr. Teplinsky emphasizes, “The more we understand the ‘why’ behind resistance, the better we can tailor the ‘how’ of treatment.”
By integrating genomic testing as a consistent element of care and clearly communicating its purpose early in the treatment journey, we empower patients to face uncertainty with greater confidence and hope. Working together—clinicians, patients, advocates, and industry—we are rewriting the story of metastatic breast cancer, one informed conversation at a time.
References
1. Zundelevich A, Dadiani M, Kahana-Edwin S, et al. ESR1 mutations are frequent in newly diagnosed metastatic and loco-regional recurrence of endocrine-treated breast cancer and carry worse prognosis. Breast Cancer Res. 2020;22(1):16. doi:10.1186/s13058-020-1246-5
2. Flaherty C. Timing of ESR1 Mutation Testing Is Critical to Overcome Adaptive Endocrine Resistance in HR+ Breast Cancer. OncLive. June 19, 2025. Accessed August 25, 2025. onclive.com/view/timing-of-esr1-mutation-testing-is-critical-toovercome-adaptive-endocrine-resistance-in-hr-breast-cancer
3. Venetis K, Pepe F, Pescia C, et al. ESR1 mutations in HR+/ HER2-metastatic breast cancer: enhancing the accuracy of ctDNA testing. Cancer Treat Rev. 2023;121:102642. doi:10.1016/j.ctrv.2023.102642
4. Tempus and Stemline Therapeutics, Inc., A subsidiary of the Menarini Group, Announce Collaboration to Implement Tempus Next, an AI-Enabled Care Pathway Intelligence Platform to Support Patients with Metastatic Breast Cancer. News Release. Tempus. February 21, 2025. Accessed August 26, 2025. tempus.com/news/tempus-and-stemlinetherapeutics-inc-a-subsidiary-of-the-menarini-group-announcecollaboration-to-implement-tempus-next-an-ai-enabledcare-pathway-intelligence-platform-to-support-patientswith-m/?srsltid=AfmBOoqKBtZse_HUBEOESM5X1h_S_ G2Lf6_OvdFlBMnHbGLAaZBiKrRt#:~:text=Up%20to%20 50,making%20decisions
5. European Commission Approves Menarini Group’s ORSERDU® (Elacestrant) for the Treatment of Patients with ER+, HER2- Locally Advanced or Metastatic Breast Cancer with an Activating ESR1 Mutation. Menarini Group. September 20, 2023. Accessed August 25, 2025. menarini.com/en-us/news/ news-detail/european-commission-approves-menarini-groupsorserdu174-elacestrant-for-the-treatment-of-patients-wither-her2-locally-advanced-or-metastatic-breast-cancer-withan-activating-esr1-mutation.html#:~:text=issued%20in%20 July%202023,been%20more%20difficult%20to%20treat
6. Burstein HJ, DeMichele A, Somerfield MR, Henry NL; Biomarker Testing and Endocrine and Targeted Therapy in Metastatic Breast Cancer Expert Panels. Testing for ESR1 Mutations to Guide Therapy for Hormone ReceptorPositive, Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer: ASCO Guideline Rapid Recommendation Update. J Clin Oncol. 2023;41(18):3423- 3425. doi:10.1200/JCO.23.00638
7. Fribbens C, O’Leary B, Kilburn L, et al. Plasma ESR1 mutations and the treatment of estrogen receptor–positive advanced breast cancer. JCO. 2016;34(25):2961-2968. doi: 10.1200/JCO.2016.67.3061
8. Brett JO, Spring LM, Bardia A, Wander SA. ESR1 mutation as an emerging clinical biomarker in metastatic hormone receptor-positive breast cancer. BCR. 2021;23. doi: 10.1186/ s13058-021-01462-3
9. Gradishar WJ, Moran MS, Abraham J, et al. NCCN Guidelines® Insights: Breast Cancer, Version 4.2023. J Natl Compr Canc Netw. 2023;21(6):594-608. doi:10.6004/ jnccn.2023.0031
10. Pascual J, Attard G, Bidard FC, et al. ESMO recommendations on the use of circulating tumour DNA assays for patients with cancer: a report from the ESMO Precision Medicine Working Group. Ann Oncol. 2022;33(8):750-768. doi: 10.1016/j.annonc.2022.05.520
11. FDA approves elacestrant for ER-positive, HER2-negative, ESR1-mutated advanced or metastatic breast cancer. News Release. U.S. Food and Drug Administration. January 27, 2023. Accessed August 26, 2025. fda.gov/drugs/ resources-information-approved-drugs/fda-approveselacestrant-er-positive-her2-negative-esr1-mutated-advancedor-metastatic-breast-cancer#:~:text=FDA%20also%20 approved%20the%20Guardant360,cancer%20for%20 treatment%20with%20elacestrant
12. Guardant Health receives FDA approval for Guardant360® CDx as companion diagnostic for Menarini Group’s ORSERDU™ for treatment of patients with ESR1 mutations in ER+, HER2- advanced or metastatic breast cancer. News Release. Guardant Health. January 30, 2023. Accessed August 26, 2025. investors.guardanthealth.com/press-releases/ press-releases/2023/Guardant-Health-receives-FDA-approvalfor-Guardant360-CDx-as-companion-diagnostic-for-MenariniGroups-ORSERDU-for-treatment-of-patients-with-ESR1- -mutations-in-ER-HER2--advanced-or-metastatic-breast-cancer/ default.aspx#:~:text=,benefit%20from%20ORSERDU%20 targeted%20therapy
13. Cancer Support Community. Cancer Experience Registry Patient Insights Report. 2024. Accessed August 26, 2025. cancersupportcommunity.org/sites/default/files/file/2025-01/ CER_PatientInsightsReport_2024.pdf