Publication
Article
Article
Author(s):


Communities across the United States—particularly rural and underserved areas—face persistent obstacles to early detection of cancer and other high-risk conditions. As a leading health care company serving diverse communities from coast to coast, Lifepoint Health understands the unique challenges and opportunities within these areas and seeks to help close gaps and increase access to care across its footprint nationwide. One example is the development of the organization's Healthy Person Program, which combines computational linguistics, standardized workflows, and nurse navigation to identify patients at risk, coordinate follow-up, and measure outcomes across a multistate enterprise. Originating with lung cancer screening and incidental pulmonary nodule management, Lifepoint's Healthy Person Program has since expanded to breast and cardiovascular cohorts and additional disease states. This article describes the program's inception, operations, results, and lessons learned, offering a replicable blueprint for community-based systems seeking to implement proactive, equitable early detection at scale.
The Challenge: Equitable Early Detection in Community Settings
Early detection saves lives, yet the benefits of preventive screening and timely follow-up remain unequally distributed. Rural hospital closures, limited subspecialty access, and fragmented care pathways create barriers that delay diagnosis and treatment. For community-based health care systems, the challenge is not merely to launch screening programs, but to build an operating model that consistently turns incidental findings into action—at every site, for every patient.
The stakes are high. When incidental findings (eg, pulmonary nodules, coronary artery calcifications, aneurysms) remain buried in radiology narratives or stall in handoffs to another provider for follow-up, patients present later when care is more complex, outcomes worsen, and costs rise. Lifepoint serves diverse communities across the country, many with constrained resources. It needed a model that would work everywhere—not just at comprehensive acute care hospitals—with consistent quality, measurable results, and financial sustainability.
Program Inception: From Healthy Lung to an Enterprise Framework
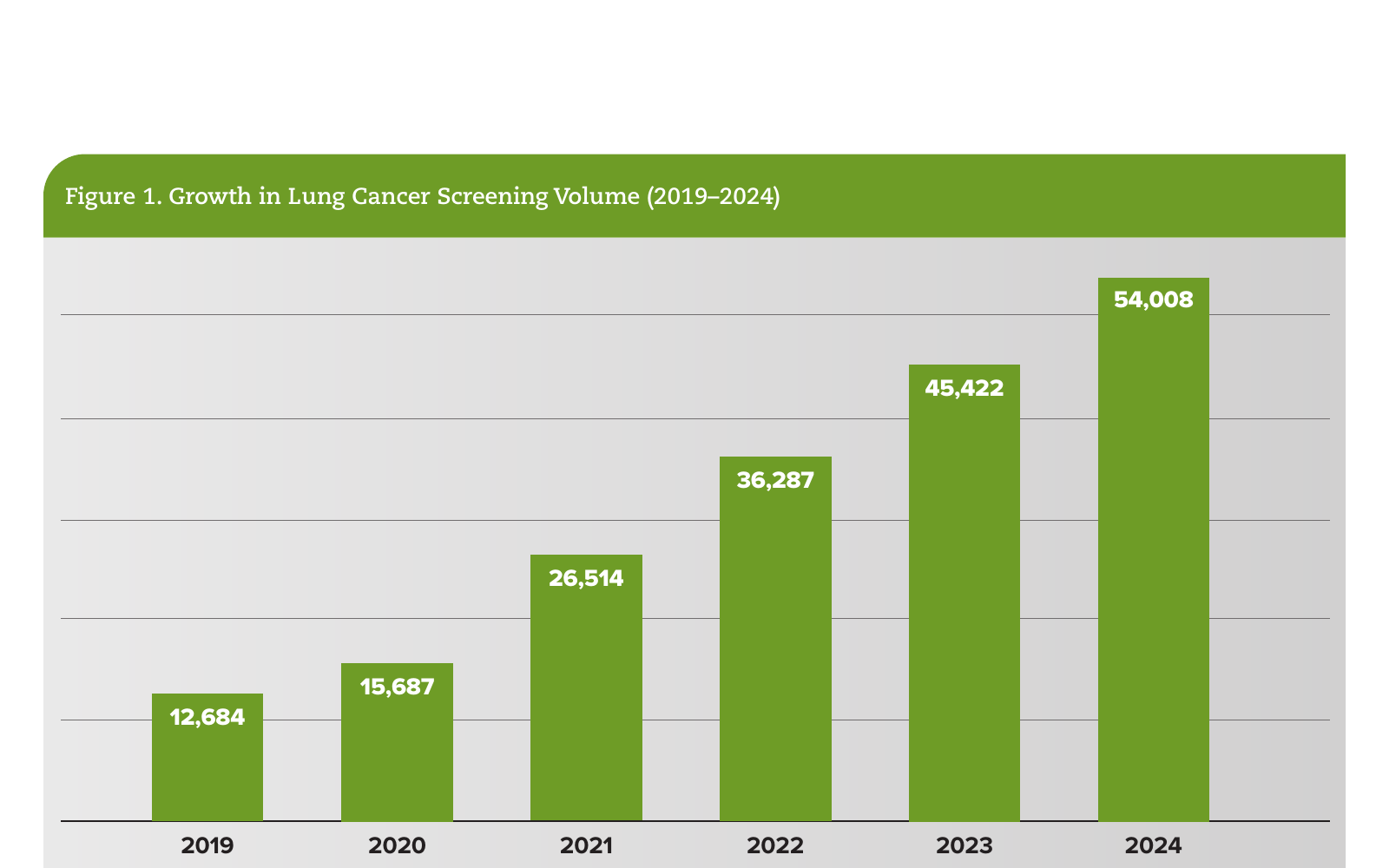
In 2018, Lifepoint launched the Healthy Lung initiative to address low national screening rates and poor adherence to follow-up for incidental pulmonary nodules. The team designed a repeatable operating model centered on 3 pillars.
As results accumulated, Lifepoint generalized this model into the Healthy Person Program—an enterprise framework that today extends beyond lung to breast and cardiovascular cohorts and other high-value conditions where early identification changes outcomes. The program's core idea is simple: Use linguistics and automation to catch what the human eye might miss, then use human navigation to make sure the patient does not fall through the cracks.

Turning Data Into Action
The Healthy Person Program integrates technology, clinical expertise, and operational discipline to convert unstructured data into coordinated care. Here's how it works.
Implementation and Governance: Standardization With Local Flexibility
The Healthy Person Program operates through multidisciplinary governance that includes oncology, radiology, primary care, nursing, IT/analytics, operations, and finance. Sites adopt the same core workflows and evidence-based guidelines while tailoring roles to local resources. Key enablers include:
Importantly, the program complements—not replaces—clinical judgment: Technology elevates the right work, while navigators and clinicians ensure the right care.
Results and Outcomes
The Healthy Person Program has driven system-level improvements in access, adherence, and outcomes while demonstrating operational sustainability. Successes include:
These results reflect the compounding effect of standardized detection, human navigation, and relentless measurement.

A Patient-Centered Safety Net: A Brief Vignette
A 67-year-old former smoker presents for an abdominal CT. The scan incidentally captures a portion of the lung base, where natural language processing flags a 9-mm nodule. Within 24 hours, the navigator contacts the patient and primary care provider with guideline-based recommendations and schedules follow-up imaging. When the nodule grows, an expedited pulmonology consult and biopsy confirm early-stage non–small cell lung cancer. Surgery takes place within 2 weeks. The patient completes treatment close to home with coordinated follow-up—an example of how standardized workflows and navigation convert incidental findings into timely, life-saving care.
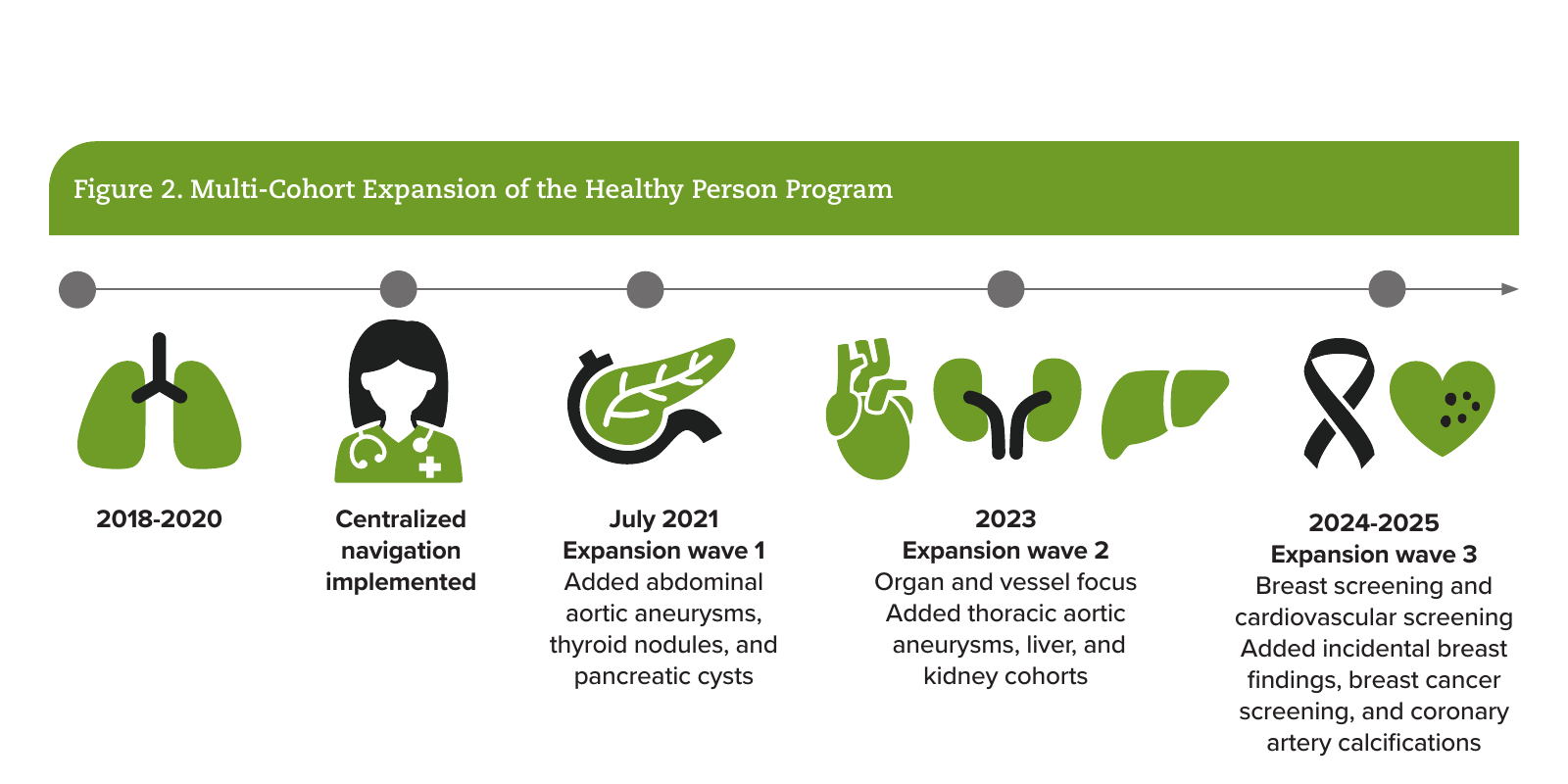
Beyond Lung: Cohort Expansion and Enterprise Synergies
The Healthy Person Program is disease-agnostic. After proving its effectiveness in lung, Lifepoint extended the model to additional cohorts (Figure 2):
Each cohort reuses the same digital infrastructure, navigator model, and measurement system—accelerating time-to-value and ensuring a consistent patient experience across markets.
Equity and Access: Meeting Patients Where They Are
The Healthy Person Program is, at its core, an equity initiative. By automating detection and standardizing follow-up, the program reduces the chance that geography, staffing variability, or documentation differences determine patient outcomes. Centralized navigation provides practical support—transportation planning, education, coverage guidance—while respectful, repeated communication helps build trust. In rural and underserved communities, this approach shifts diagnosis to earlier stages and improves continuity across local settings of care.
Future Directions
For 2026, Lifepoint targets screening of approximately 20% of the eligible lung population and an additional approximate 8% increase in breast cancer screening among eligible patients. Looking toward 2030, the Healthy Person program aims for 100% follow-up on high-risk findings and continued cohort expansion. To support this growth, Lifepoint is investing in:
Operational Lessons Learned
In 2025, Lifepoint was awarded an ACCC Innovator Award for its Healthy Person Program. For organizations looking to set up a similar enterprise-wide, AI-driven program, Lifepoint suggests starting small and designing for scale. Select an initial cohort (eg, lung) with clear guidelines and measurable outcomes. Define governance early and build a navigator-led workflow with technology support. Measure adherence and time-to-treatment from day 1. As outcomes improve, reinvest in navigation capacity and analytics. Most importantly, cultivate a culture that treats incidental findings and screening follow-up as core safety practices, not "extra work."
A practical starter kit might include:
Figure 3 offers a visual road map for cancer programs to follow.


Concluding Thoughts
Lifepoint's Healthy Person Program demonstrates that proactive, data-driven, early detection can be delivered reliably in community settings at scale. By uniting linguistics, navigation, and standardized workflows within a disciplined governance model, Lifepoint Health has created a durable safety net that changes the trajectory of disease for thousands of patients. The blueprint is replicable: Start with focused cohorts, align technology and people, measure relentlessly, and expand thoughtfully. In doing so, health systems can improve outcomes, reduce disparities, and make every community healthier.
Bart Daugherty is vice president of Clinical Technology and Systems at Lifepoint Health, where he leads enterprise programs spanning clinical imaging, navigation, and AI-enabled analytics focused on early detection and follow-up. Chris Frost, MD, is senior vice president, chief medical officer, and chief quality officer at Lifepoint Health. Dr Frost oversees clinical quality, patient safety, and physician engagement across Lifepoint's national network, with a focus on value-based, patient-centered care.



: A Proven Framework for Streamlined Cancer Care Delivery")












