Author(s):
Lung cancer remains the leading cause of cancer-related death in the United States, accounting for more fatalities than colorectal and pancreatic cancer combined. One of the keys to improving clinical outcomes lies in early detection and intervention, especially for incidental lung nodules, which could be an early indicator of lung cancer.
Lung cancer remains the leading cause of cancer-related death in the United States, accounting for more fatalities than colorectal and pancreatic cancer (the second and third leading causes of cancer-related death), combined.1,2 As the third most frequently diagnosed cancer type in the US, lung cancer is quite common with an estimated 234,580 new cases diagnosed annually.2 Unfortunately, many cases of lung cancer are diagnosed at a late stage, resulting in poor survival rates. However, when detected early, the 5-year relative survival rate increases dramatically from 9% to 65%.3 One of the keys to improving clinical outcomes lies in early detection and intervention, especially for incidental lung nodules, which could be an early indicator of lung cancer.
In response to this significant need, Princeton Cancer Canter at Penn Medicine Princeton Health decided to leverage cutting-edge AI technology to better serve their patient population. Although they are part of the University of Pennsylvania Health System, their location in New Jersey leads them to serve as a community hospital. As such, the institution interfaces with hundreds of independently practicing physicians, with many different referral patterns that can be difficult to manage in a systematic manner. In an effort to streamline patient care, the first use of AI at their institution involved a tool capable of text-mining all pathology reports processed at the centralized lab. In this way, all new cancer diagnoses were routed by AI to a nurse navigator who ensured appropriate follow-up was carried out.
With the success of their pathology report text-mining AI tool, extending similar technology to radiology reports was a logical next step. After 6 months of strategic planning with the AI algorithm creator and careful coordination with information technology and compliance, the lung nodule screening program was ready for implementation.
The multidisciplinary steering committee responsible for the program’s implementation consisted of experts from pulmonology, medical oncology, radiology, thoracic surgery, nurse navigation, and hospital administration. Together, it was decided that all radiology reports of chest imaging ordered in the emergency department (x-rays, CT scans, MRIs, etc) would be routed to the AI lung nodule detection tool. This was a strategic choice, as patients seeking care in the emergency department are less likely to have a primary care physician whom they see regularly. This patient population is at a higher risk of “falling through the cracks” and not receiving appropriate follow-up care. All positive reports (with identified lung nodules >8 mm in size) are then forwarded by the AI tool to the oncology nurse navigator.
The oncology nurse navigator is alerted to approximately 20 new patients per month with incidental lung nodules noted on radiology reports. From there, the nurse navigator investigates if the patient is aware of the nodule, verifies if they have received appropriate follow-up care, and obtains any prior imaging for comparison purposes (as needed). This process narrows the patient list down to about 10 patients, who are forwarded to the pulmonologist for further review. Ultimately, 5 or 6 patients are identified as having new, incidental lung nodules requiring follow-up care and additional workup.
Once a month for 30 minutes, the multidisciplinary team meets to review imaging and decide on the most appropriate next steps of care (eg, CT, PET scan, biopsy). The nurse navigator then contacts the patients, briefly explains the clinical context and screening process, and schedules appointments with the appropriate specialists.

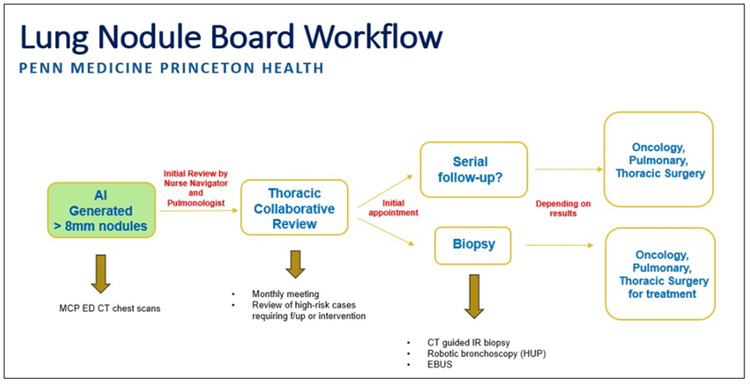
Image used with permission
Since the start of the Lung Nodule Screening Program, the following results have been achieved:
This early success highlights the potential of the program to achieve early diagnosis and timely intervention for patients who may have otherwise presented at an advanced stage of disease. Although the AI technology used for lung nodule screening does require significant upfront cost, the follow-up care and early intervention not only save lives but also provide a strong return on investment for cancer centers. Long-term costs associated with treating advanced-stage lung cancer are also reduced.
The AI-assisted Lung Nodule Program at Princeton Cancer Center is a model for the future of lung cancer screening and early detection. By combining cutting-edge technology and a dedicated multidisciplinary team, the program offers a blueprint for quality cancer care. As the Director of Cancer Services at Penn Medicine Princeton Health, Kerri Celaya, MA, FACHE, is happy to share insights driving the success of the Lung Nodule Program for other cancer centers looking to initiate similar screening efforts. She can be reached at kerri.celaya@pennmedicine.upenn.edu.